Some people I meet in clinic look a little embarrassed when I ask them where they are from. The population of southern Utah is growing rapidly, fueled mostly by an exodus from California. Some of the old locals here are upset about how congested our quiet little town has become and are worried that the people from California will bring their “California ways” with them.
I don’t think they have much to worry about. The people moving here are more like refugees than colonists. In a place where every other vehicle on the road is a pickup truck, and where in election years a lot of them are decked out with MAGA flags, the newcomers more or less fit right in. You don’t move here if you want to live in a politically progressive stronghold.
Here is a typical conversation I might have with a new patient:
ME: How long have you lived here?
PATIENT: Since 2021.
ME: Do you like it here? Are the locals nice to you?
PATIENT: I love it! Our neighbors are wonderful.
ME: Where did you move from?
PATIENT: Southern California.
ME: I used to live in Bakersfield a long time ago.
PATIENT: Oh, I’m sorry.
ME: [Shrugs shoulders and smiles.] Bakersfield is not the kind of place you miss much when you move away. We went to St. George when I was 15 years old. It’s a little hotter in St. George, but the scenery is gorgeous, the air is clean, and the water doesn’t taste like crude oil!
I have had a conversation like this a few times every week for the last several years. (For the record, Bakersfield wasn’t really such a terrible place to live, but its armpit-of-the-state reputation makes for easy small talk.)
There are two kinds of people that live in southern Utah: descendants of the pioneers, and imports from California (or Vegas). Those two groups make up probably 95% of the people who come to my clinic, and because I happen to be in both categories, I can get along with anyone.
When it comes to the old-timers, I know their history and I understand their religion. I am one of them, so they can trust me. Some of them are even my distant cousins. And when it comes to the move-ins, I can understand them too because I have lived where they are coming from and I know what it’s like to move in to this beautiful state with its wonderful and quirky people.
When I first walked into the hospital administrator’s office on my interview day, I noticed a beautiful landscape photo hanging on his wall.
“Is that Snow Canyon?” I asked.
“I can tell you’re a local,” he said.
I was a shoe-in.
During that job search in 2015 I looked at multiple positions in Utah and the surrounding western states. I had a phone interview with a neurologist who was recruiting a partner for his clinic in one of the cities along the Wasatch Front. In the course of our conversation he divulged that he was planning to leave the job soon, and I asked him why. After hesitating, he said, “That’s a fair question. I’m not from here, and I find the local culture … a little overwhelming.” I knew what he was talking about. It takes a cultural insider to really thrive here.
There is a reasonable argument that health care providers should reflect the diversity of the populations they serve. It seems logical to assume that a cultural insider would be able to connect with and counsel patients in a way that an outsider could not do as easily. This idea is supported by population health research, and is thought to be part of the reason why minority groups can have poorer health outcomes than majority groups served by the same health system.
I think that any open-minded and respectful professional could be a good doctor in my town, even if they don’t have family or religious or geographic ties to a specific patient they are seeing. A doctor who really cares about helping patients could provide high quality health care for people who speak a different language or believe in different things. But it does help if you have a head start on all of that.
I’m not exactly a “diversity hire.” My ancestry is exclusively northern European, and I have a Y chromosome. American English is my native language (although I understand British English pretty well too). My politics are fairly conservative (but not Trumpy). A corporate DEI officer wouldn’t put my CV at the top of the stack. And yet I am an almost perfect match for the community I serve.
I am also a good neurologist, which I think comes well before any of the identity-based qualifications I might have. If I were an incompetent or a malevolent doctor, then any good and honest neurologist would be better than I am at serving the needs of this community, regardless of how deftly they could navigate the quirks of our local culture. In other words, I would rather have a doctor that really knows medicine and is so-so on my culture than a doctor who really groks my lived experience but who couldn’t pass a board exam.
Doctors should make reasonable efforts to have cultural competency for the population they serve. For example, as far as I know there is not a neurologist anywhere who is a member of the Paiute tribe, so it falls on me to care for the local Paiute patients. On several occasions I have asked a Paiute tribe member to tell me about their community. Would it make me a better doctor if I did more to study their history or attended their pow-wow? I think those things would be interesting to do, and it would likely help me connect with some patients, but it probably wouldn’t make me any better at secondary stroke prevention.
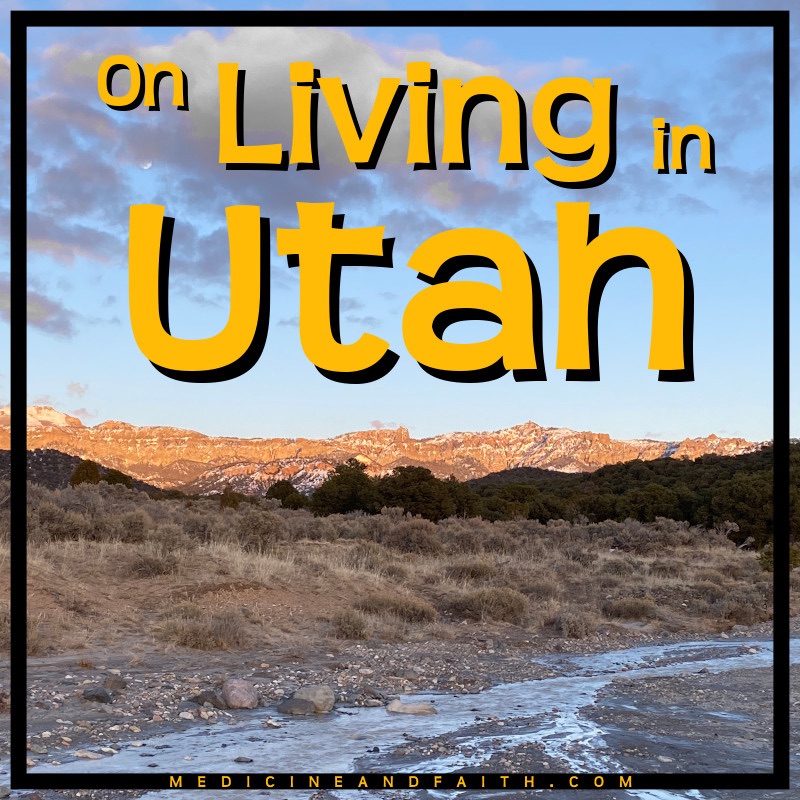
Utah is a wonderful place to live and work. Just yesterday I went for a six mile trail run after clinic and gawked at the red and white cliffs shining in the evening sun. At about three miles the sun went down, and at mile four I saw the nearly full moon in the deep blue sky above the cliffs, now darkening into a slate grey. The runner’s high was tickling my brain chemistry, and I could not restrain myself from praying out loud: “I am so grateful to be here in this beautiful place!”
I love the people of southern Utah — all of them: the old-timers with their old-time accent, who have farmed and ranched in these hills and valleys for all of their lives, and who have loved God and taught their children to love God; the liberty-loving Californian exiles who are here for elbow room and peace; the Paiutes who have a sense of local history that goes back well before 1847; the young people who are working and building their homes and businesses and families; the fundamentalists from Colorado City who are less afraid of us than they used to be, and everyone in between — even the MAGA flag crowd. It is a privilege to live here with them, to serve them, and to be one of them.
Alan B. Sanderson, MD is a member of The Church of Jesus Christ of Latter-day Saints and is a practicing neurologist.

Best one yet! You’ve hit your stride and are winning.
LikeLiked by 1 person
Alan, I liked the perspective “Doctors should make reasonable efforts to have cultural competency for the population they serve”. As a physician who is working (locum tenens Neurohospitalist) out in a Neurology desert (in a verdant, not arid climate), I can speak from experience that this THE most important skill (assuming competence in one’s area of expertise) to be effective in the delivery of care. It serves to answer my natural curiosity about diverse perspectives, too. Carry on, old friend—it’s a journey as the foundation of wisdom.
LikeLike
Thanks, JohnofOhio! Anthropology was one of my pastimes when I worked in Ohio. I loved the people out there too — especially the ones from Appalachia.
LikeLike
We’ve both lived in California and now have places in Southern Utah. I’m sure you’re right that being competent is more important than being culturally clued in, but the culture helps. I love hikes in Southern Utah too.
LikeLike
When I was an intern my mantra was “competency before efficiency.” Now I think competency should come before pretty much everything else in medicine.
LikeLike