
This article is the fourth of a six-part series, written in the hope that it will be useful to those who are considering or preparing for a career in medicine, and at least entertaining and uplifting for the rest of you:
- First Decisions: Deciding to become a doctor
- Apply Yourself: Undergraduate studies
- The Academic Eating Contest: Medical school preclinical years
- Academic Vertigo and the Identity Crisis: Clinical rotations and specialty choice
- Keep Your Nose Above Water: Surviving residency
- Living the Dream: The transition from training to practice
My life changed abruptly and irreversibly in July of my third year, when I started my first clinical rotation in the hospital. This gave me my first opportunity to see how hospital teams function, and what role doctors play on that team. I remember the “A-Ha!” moment when I first comprehended the difference between what doctors do and what nurses do. (Recall my breathtaking ignorance described in Part 1 of this series.)

Every month or two for the next two years I rotated through a different type of practice. I started with internal medicine, then surgery, then family medicine, psychiatry, neurology, pediatrics, obstetrics and gynecology, radiology, addiction medicine, emergency medicine, etc. Every month (and sometimes every day) I had a new team of doctors and residents to work with in an entirely different hospital or clinic setting. As soon as I got my bearings and felt like I knew what I was doing, it was time to move on to something else. In addition to these frequent changes of venue, I also found that I was no longer in charge of my own schedule like I had been for many years. Weekend and overnight work assignments were frequent. Even when things are going well this sort of instability is stressful.
But equally important to this lifestyle change was the more subtle transformation which started to happen in myself. I was no longer just a student, as I had always been since I started Kindergarten; I was now becoming a clinician. This represented a change not only in what I was learning, but also how and why I was learning it. Textbooks and lectures became a supplement to what I was learning from real patient encounters instead of the primary focus of my learning. And when I consulted a book or other reference it was with the intent to use that knowledge in a clinical context, or to understand more fully what I had just observed.
During the second half of medical school I had many experiences which changed my life forever. My very first hospital patient had a new diagnosis of HIV infection, and presented to the hospital with AIDS. I also saw living anatomy in the operating room, hallucinations and delusions on the psychiatry ward, death on the oncology ward, and withdrawal on the acute detox ward. One of the most rewarding experiences in all of medicine is to deliver a new baby to a grateful mother.
Not all of the changes were for the better. The culture of medicine includes a unique and dark humor, laced with sarcasm and cynicism. Clinical rotations were my first real immersion experience in this strange culture, and by the end of my third year I was starting to understand it and participate in it. The full expression of this dark side of medical culture won’t blossom fully until halfway through residency for most trainees, but hardly anyone escapes medical school without picking up some of it. During my pediatrics rotation I drew a comic showing a man with his head cut off. This would probably have shocked me at an earlier point in my life, but my classmates and the residents on my team just roared with laughter when I showed it to them.
Cynicism is not a benign or incidental feature of medical culture. It is one of the cardinal symptoms of occupational burnout, and the fact that it is so entrenched in our culture speaks volumes about how common burnout is among physicians. From the perspective of an idealistic student who signed up to be a doctor so that he can help and serve people, this cultural experience can be very jarring. It may be your first warning that practicing medicine in the real world may not be quite what you imagined it to be.
Two Steps Forward
The United States Medical Licensing Examination (USMLE) Step 2 is normally taken during the first part of year 4 in medical school. This is a two-part exam, including a computerized multiple choice examination (Clinical Knowledge, or CK) and a practical examination (Clinical Skills, or CS). Step 2 CK is very much like Step 1 in its format, length, and difficulty, but the subject matter is clinical rather than basic science. A couple of weeks before I took Step 2 CK I was studying out of a review book, doing practice exam questions for obstetrics and gynecology. After an hour or so I got sick of reviewing questions, so I decided to write my own:
Which of the following statements is not truly false on opposite day?
-
- This question is easy
- You are a green monkey
- None of the above
- This question is poorly worded
Step 2 CK is administered at hundreds of different testing centers, so you probably won’t have to travel far to take it. Step 2 CS, on the other hand, usually requires traveling to a testing center unless you happen to live in one of the five cities where it is administered. I took mine in Chicago, spending the night in a cheap motel the night before. (Apparently “non-smoking” meant that I, as the guest that night, would not be smoking. The whole room reeked of tobacco, and so did I after sleeping there.) Any reasonably intelligent medical student who speaks fluent English should be able to pass Step 2 CS. I remember complaining at the time that I shouldn’t have to spend over $1000 of my own money just to prove that I can speak English. Maybe I’m still a little resentful about that.
A Place in the Sun
When I started medical school I had no idea what specialty I might choose, and the thought hardly crossed my mind until I started the third year. This is not unusual; less than half of my classmates started medical school with a specific specialty in mind. As I rotated through the many different specialties, in different hospitals and clinics every month, I often wondered where my place was in this complex machine. Where can I make my contribution? Where do I belong? What specialty should I choose?
On every rotation I would ask my attending physician why they chose their specialty and whether they would choose it again if they had to start over. This is a very simple exercise which I recommend to every medical student, because if you pay close attention to the answers you will learn a lot about what things are important to a practicing doctor. You will learn which personality traits are attracted to which specialties, and why, and you can compare that to what you feel is important to you. Along the way you will hear something that will really resonate with you, and that will be a clue that you have found what you are looking for, or at least that you are close. Another clue is when you find yourself thinking of how nice it would be to work for the rest of your career with people like the ones you are working with that month.
Some rotations were easier than others, and some were more interesting than others. One of my favorite months was spent with a solo family practice doctor, taking Thursdays off every week and getting home before 5:00 every day. My wife said, “Can you please get a job like this one?” But there were many months with oppressively long hours, and many months of working with people I didn’t really get along with. Sometimes it was hard for me to see a bright future for myself.
During the early springtime of my third year, at the end of a cold and long Midwestern winter, I was driving to the children’s hospital for another day on a rotation that I didn’t really like. I was listening to an old Stevie Wonder album, and when “A Place in the Sun” came on it seemed like Stevie was speaking right to me: “You know, when times are bad, and you’re feeling sad, I want you to ALWAYS remember: Yes, there’s a place in the sun, where there’s hope for everyone […] And before my life is done, gonna find me a place in the sun.” This song gave me hope that I was not wasting my time in a failing effort. There was a light at the end of this tunnel, and I felt determined to keep marching forward until I found it.
I still cry sometimes when I listen to that song.
A Thinkin’ Doctor
The first big question every medical student needs to decide is whether or not they are a surgeon. One of the neurosurgeons I worked with during my training used to say to his patients, “There’s two kinds of doctors: cuttin’ doctors and thinkin’ doctors.” If he felt that the patient’s problem was non-surgical, he would say, “Now, I’m a cuttin’ doctor. What you need is to find yourself a thinkin’ doctor.”
The operating room is a fascinating place, but it didn’t take me very long to decide that I didn’t like the surgery lifestyle. At the time of my first surgery rotation I already had a wife and three children, and during the first week of the rotation I rarely saw any of my kids awake. I got the feeling that if I became a surgeon it would make me an absentee father, which I didn’t want to be. Also, I didn’t see myself as a very good fit in the surgery subculture. So the first question was answered: I am not a surgeon.
The previous paragraph merely documents my own personal decision process, and is not meant as advice to anyone that they should avoid careers in surgery. I personally know many reasonable and family-oriented people who are surgeons, and I am so glad that there are good people in this world who want to be surgeons (so that I don’t have to).
A friend of mine is currently a nontraditional student in her last year of medical school, and recently she told me about her specialty choice: “I really tried to like other specialties more than surgery, but, kind of like going to medical school, I couldn’t let go of surgery. It’s what I’ve wanted to do since I was 5 years old. But given my age, I thought I’d better look into other possibilities. Nothing draws me in like surgery, though. When people would ask me, ‘What do you want to be when you grow up,’ the answer was always, from 5 years old, ‘A cardiovascular surgeon.’ (The dumbfounded looks I got were priceless!) I don’t know that cardio, or vascular, or thoracic surgery is the way I’ll end up going, but I decided I need to do what makes me happy. That’s why I went to medical school in the first place.”


Decision Time
The second question was harder to answer: how do I choose from among the non-procedural specialties? It turns out that the only way to answer this is the Goldilocks method: try them each until you find one that is just right. And you only have about a year to decide because the residency application takes up most of the fourth year of medical school. But don’t worry; by the time you really have to make the decision you will have all of the data you need.
My own informal survey of the major specialties gave me the following impressions: Internal medicine doctors like the challenge of figuring out a puzzle and managing a complex case. Surgeons like to fix things. Family medicine comes in two varieties: 1) Brilliant minds who just can’t bring themselves to exclude anything and want to dabble in it all, and 2) Less than brilliant minds that couldn’t match into a more competitive specialty. Emergency medicine doctors are adrenaline junkies. Obstetrician/gynecologists love the combination of surgery and internal medicine. Pediatricians … I don’t know. They never made sense to me. Psychiatrists are all a little bit crazy. Neurologists are circuit geeks. Radiologists are technology geeks. Pathologists are just geeks.
As I approached the end of the third year my short list looked like this: 1) Family Medicine, 2) Neurology, and 3) Psychiatry. I liked the patient-centered approach of family medicine, and I liked the idea of seeing and doing a bit of everything. I liked psychiatry because of the fascinating symptoms, but I ultimately scratched it off of the list because I didn’t want to leave behind the entire world of general medical conditions, and I figured that I would see a lot of psychiatry in the other two specialties anyway. Neurology included everything I liked about psychiatry, but was grounded in definable pathophysiology and also included the fascinating game of neurologic localization. But I wasn’t sure whether I wanted to specialize in just one organ system, as cool as it was.
Obstetrics and gynecology was my last rotation of third year, and at the beginning of the month I was leaning towards family medicine. But after a couple of weeks I realized that family medicine residents have to rotate through ob/gyn, and I never wanted to see that specialty again. So neurology it was!
Seeing Myself for the First Time
And once I had made my decision I saw my life flash before my eyes. I remembered how fascinated I was with neuroanatomy and neurophysiology in my undergrad classes. I remembered my neurophysiology course during the first year of medical school, and how much I regretted that I didn’t have time to read the whole 1300-page textbook.
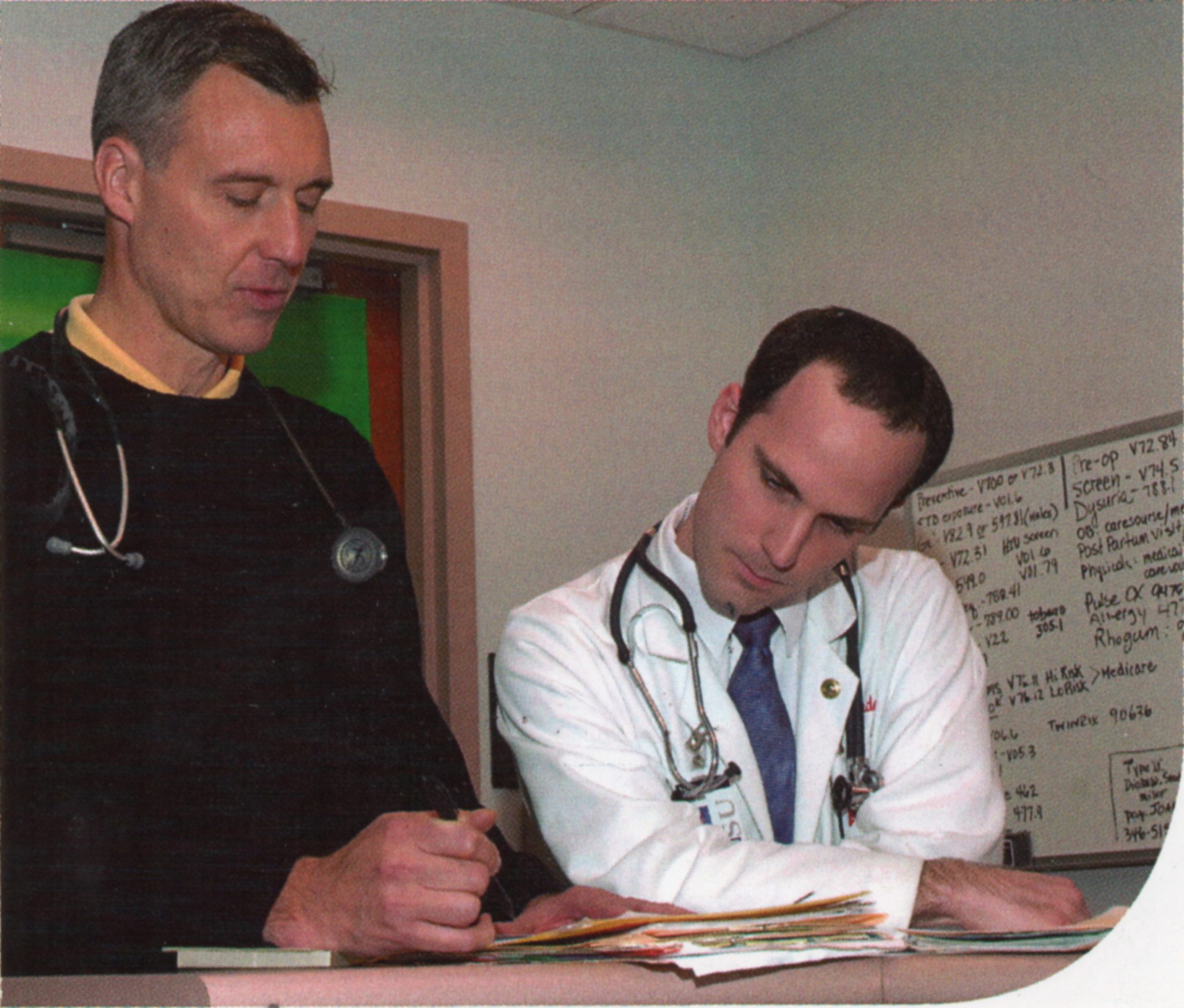
During my third year neurology clerkship I saw a patient who had just had a brain tumor removed. When I walked into the room and greeted him he said, “I need to get it on the shelf,” and he gestured towards his right side. Confused, I asked him a follow-up question and got an equally nonsensical answer. Suddenly I realized that he had Wernicke’s aphasia, a condition I had read about but never seen until that day. I thought again about the MRI I had just reviewed, and I felt a terrible thrill when I realized the patient’s tumor was right next to Wernicke’s area! As I walked back to the neurology offices to report on what I had seen my feet barely touched the floor.

I stopped by the office of the neurology clerkship director and excitedly said, “I just saw Wernicke’s aphasia for the first time!” We talked for a few minutes, and she could easily see that I was interested in neurology. I told her about the time I had found my neurophysiology textbook while unpacking a box and how I couldn’t help but read a chapter or two. She looked at me sideways, and I shrugged my shoulders and explained defensively, “It was about the higher-order cortical processing of vision. It was just so fascinating!”
“Alan,” she replied, “You can’t ignore stuff like that.” And she was right. Neurology was my destiny.
Make Me a Match
I applied to thirteen neurology residency programs and was offered interviews at all but one. The first interview invitation I received was this email:
Thank you very much for you [sic] application to the Neurology Residency Training Program at _______ University Medical Center. We are pleased that you have chosen to consider our program. The review of your application is now complete and the conclusion of the faculty is very favorable and we are pleased to extend you an invitation for interview. Please contact my office at your earliest convenience to make arrangements for a visit.
Again, thank you very much for your interest in our program. We look forward [sic] meeting you in the near future.
Sincerely,
Dr. X, Residency Director
Dr. Y, M.D., Ph.D., Professor and Chair
I was very pleased to get this email. The run-on sentence in the first paragraph and the missing word in the last sentence were a bit concerning, but maybe they were so eager to invite me that they forgot to proofread their email. Maybe this wasn’t just a form letter, but was actually composed that morning by Dr. X, with Dr. Y reading over his shoulder and making small suggestions here and there. “We can’t waste any time with this one, Dr. X. He’s got to be invited immediately.”
“Agreed, my most esteemed colleague.”

Interviewing for residency is a very different experience compared to interviewing for medical school. The dark suits are the same, but the crowds are smaller. Every program will take you out to eat on the night before your interview, and a few will even put you up in a hotel for the night. They will do more to make you want to choose them.
Residency interviews will teach you a lot, if you pay attention and take good notes. Of course you will learn about the different programs and what they have to offer, but you will also learn about yourself in the process. What things are really important to you? Do you want to live in a big city or a smaller town? Are you willing to tolerate a frequent overnight call schedule, or would you rather go to the program that has a night float system? Do you want a department that has all of the subspecialties represented, or do you want to learn from a smaller number of generalists? After visiting about five or six programs I thought I had found what I wanted, and interview fatigue started to set in as I completed the rest of the visits.
Your experience will differ markedly depending on what specialty you have chosen. If you are a brilliant mind who wants to do family medicine, then you will have many excellent programs to choose from. If you are a less than brilliant mind who wants to do dermatology, then you will be more of a beggar than a chooser.
Residency applications are filtered through a computer algorithm known as the National Residency Matching Program, or simply “The Match.” Applicants submit an ordered list of their preferred programs, and residency programs submit an ordered list of their preferred applicants. The algorithm tries to find a balance between the preferences of applicants and residency programs, and it works out pretty well for most everyone. A certain number of applicants end up not matching into any program on their list and a certain number of programs end up not matching an applicant to fill up all of their slots. Thus begins a secondary process, referred to as “The Scramble,” where applicants desperately try to get into open residency slots, and residency programs frantically try to locate and recruit unmatched applicants to fill their open slots.
The Pruning
Every spring on Match Day the results are announced. Medical schools usually have some traditional way of announcing the results, often by having the students all in one room opening their letters at the same time. As Match Day approached I was feeling very optimistic. There were three programs which I really liked, and I felt certain that I would match in one of them. I started to emotionally detach myself from my surroundings, anticipating a move to a different city in a few months. We even contacted a real estate agent in the town where my favorite program was located. I had always assumed that I would go somewhere else to do residency. During my four years of medical school I felt like a transient, and I honestly never considered the possibility that I might want to stay at the same university for residency.
Imagine my surprise when I opened the letter on Match Day and discovered that I would not be moving for at least another four years. I couldn’t believe my eyes, and had to read it over again two or three times before it started to sink in that I would be staying at the same university. Cheers were erupting all around the room as my classmates opened their letters, but my wife and I sat in stunned silence.
After a minute I said, “Let’s get out of here,” and we started walking up the aisle towards the exit. Halfway up the aisle I was accosted by my exuberant neurology mentor, who was so excited that I was joining her department. I tried to show her some enthusiasm, but I wasn’t very convincing, and as I left the room I felt guilty for being so obviously disappointed.
Over the next few days I did a lot of soul-searching. What did I really want, and why did I think I wanted it? What was really important, and what were my goals? I tried to bend my brain around a new future which I had never imagined, but which would nevertheless become my reality.
My neurology mentor contacted me a day or so later, and invited me to stop by her office. We had a good conversation and she gave me some of the best advice I have ever received. She encouraged me to unpack my suitcase, as it were, and to engage with my colleagues and my workplace as if I would live in that town for the rest of my life. And again, she was right. This was exactly the right thing for me to do, and I found it very therapeutic to change my perspective in this way. In fact, I took her advice so much to heart that it was difficult for me to leave the place seven years later (but that is a story for another post).
God is the Gardener
Around that time I remembered a story I had heard many years before, called The Currant Bush, written by Hugh B. Brown. It is a parable from his own life about accepting the Lord’s will when our hopes are dashed and our aspirations are cut short. He recalled a time when he pruned back an overgrown currant bush, and had an imagined conversation with the bush about how one day it would thank him for cutting it back. Some years later this conversation came back into his mind when he was bitter about an unfair treatment he had received in his military career, as he was denied a rank promotion which he rightfully deserved. As he complained to God about his situation, he remembered his own words to the currant bush as if they were a message from the Lord: “I am the gardener here. I know what I want you to do.”
This episode of disappointment actually led him to opportunities for growth and service that he would not have had if he had gotten his wish, and he could see how this experience stopped him from making mistakes that would have negatively affected him and his children. He concluded, “And now, almost fifty years later, I look up to him and say, ‘Thank you, Mr. Gardener, for cutting me down, for loving me enough to hurt me.’” (My paraphrasing doesn’t do the story justice; it is worth your time to read the original.)
I can say the same about my time in the Midwest, where I ended up living for longer than I have lived in any other place. Five of my children were born there, and our years were enriched with wonderful friendships and great opportunities to serve. The professional training I received was solid, and prepared me well for my current work.

Over the next few months my wife and I bought our first home, and our first lawnmower. We signed the closing documents for the mortgage on the same day that I graduated from medical school. This diploma had been my goal for the previous eight years. The end of medical school was the light at the end of tunnel, and I had reached it! I now had letters behind my name, and I was starting to feel like I really belonged somewhere. Life was good, and I felt like God was blessing me and guiding me in the direction he wanted me to go.
Related Posts

First Decisions
Part 1 of a medical education memoir: Deciding to become a doctor.

Apply Yourself
Part 2 of a medical education memoir: Thoughts and memories about undergraduate studies and applying to medical school.

The Academic Eating Contest
Part 3 of a medical education memoir: Thoughts and memories about the first two years of medical school

Keep Your Nose Above Water
Part 5 of a medical education memoir: Stories and memories from the dark days of internship and residency

Living the Dream
Part 6 of a medical education memoir: Adventures and lessons from my first years in practice

Thank you for sharing your adventure. All of us experience changes in direction that take our lives somewhere other than we had originally planned, and it takes faith to accept the new direction and continue working towards our worthy goals.
LikeLiked by 1 person